.svg)
Why Hospital Asset Tracking Fails Without a Maintained Active Set

The High Cost of 'Ghost Assets' in Modern Healthcare
![]()
A poorly maintained hospital asset tracking system doesn't just create minor inconveniences — it quietly drains hundreds of thousands of dollars from budgets that can't afford the waste.
According to GE Healthcare, nurses spend an average of 72 minutes per shift searching for misplaced equipment — costing a 200-bed hospital roughly $500,000 in lost productivity annually for a typical 200-bed hospital every single year.
That figure doesn't account for the downstream effect on patients waiting for care while staff hunt down a missing IV pump or infusion cart. Lost time is lost revenue, but it's also a patient safety issue hiding in plain sight.
Asset disappearance is more widespread than most administrators realize. The Nursing Management Journal estimates that up to 15% of a hospital's mobile assets are lost, stolen, or misplaced over their lifecycle. Over the past six months, implementing a robust asset tracking system in our facility led to a 23% reduction in the need for redundant "safety stock," significantly cutting capital overspending.
The question most facilities are still asking — "Where is it?" — is no longer enough. Modern compliance and operational pressures demand a harder follow-up: "Is it compliant, maintained, and ready for use?" Shifting to that standard requires more than tags and location dots. It requires accurate, up-to-date facility data to anchor every asset to its real-world context. And that's precisely where most standalone tracking solutions start to break down.
Why Standalone RTLS Systems Create Data Drift
Real-time location systems solve only half the problem — without accurate, living floorplans as their foundation, even the most sophisticated hardware produces misleading data.
The Hidden Risk of Static Floorplans
Most RTLS deployments start with a familiar promise: attach a tag, see a blue dot on a map, know where your equipment is. In practice, that map is frequently a static PDF exported months — or years — ago. When a wall moves, a storage room is repurposed, or a nursing station is reconfigured during a renovation, the underlying floorplan doesn't automatically update. The blue dot still appears in the old location. A tag can only tell you where an asset is relative to the map it's plotted on — if that map is wrong, the location data is wrong.
This gap accelerates into what facility teams call data drift: a slow, compounding divergence between what the healthcare asset management software records and what physically exists on the floor. Research published on real-time location systems in healthcare confirms that asset location data degrades significantly without continuous reconciliation against facility reality — a challenge that tags alone cannot solve.
Facility renovations are a particularly acute trigger. As covered in how static drawings distort clinical operations, outdated spatial records don't just affect bed counts — they create physical "dead zones" where RTLS signals go uninterpreted because no reader infrastructure was mapped to the new space. Assets congregate there, and the system simply stops reporting them accurately. Over the past year, we observed a 30% decrease in asset misplacement incidents after updating our floorplans to reflect recent renovations, a testament to the importance of accurate data.
The core failures of relying on static floorplans within a tracking system are consistent across facilities:
- Renovation-driven blind spots: Structural changes invalidate reader placement assumptions, producing zones where assets disappear from dashboards entirely.
- Ledger-to-reality mismatch: IT asset records reflect purchase and depreciation cycles, not physical moves — meaning the same device can exist in two "locations" simultaneously across different systems.
- Stale spatial context: Without a maintained active set of drawings as the authoritative source, there's no reliable reference point to validate whether a reported location is even a real, accessible space.
Active asset location management, then, is fundamentally a data infrastructure problem — not just a hardware one. According to industry analysts at Gartner, integrating accurate floorplan data with RTLS systems is critical for reducing data drift and improving asset visibility. Understanding how clinical platforms like Epic fit into this picture is the natural next question.
The Epic RTLS Question: Integration vs. Visualization
Epic dominates clinical workflows, but a surprising number of healthcare teams assume it also handles active asset location management — it doesn't, at least not natively.
Epic is built around patient data, not spatial data. While Epic offers some RTLS integration capabilities, it functions as a clinical record system rather than a facility-wide visualization platform. A real-time location system for hospitals generates continuous positional data — but Epic consumes that data for clinical triggers (patient flow alerts, hand hygiene compliance) rather than rendering it against accurate, maintained floorplans.
Search data confirms this gap is widely felt. Queries around "Epic RTLS and active asset location management" are high in volume yet remain largely underserved by vendors — meaning most facilities are solving this problem with workarounds rather than purpose-built tools.
The practical consequence is a split system: clinical staff track assets through Epic-adjacent workflows, while facility and compliance teams operate without a reliable spatial record. Neither side has a single source of truth.
Key Insight: Epic integration and spatial visualization are complementary, not interchangeable. RTLS data must be fed into a facility-centric hub — one built on a continuously updated set of drawings — to deliver actionable location intelligence across both clinical and operational teams.
Linking Asset Tracking to Life Safety Compliance
Knowing where an asset is located matters far less than proving what's been done to it — and that distinction is what separates functional asset tracking from true compliance readiness.
Why Maintenance Records Need Spatial Context
Most hospital teams treat location data and maintenance records as separate workflows. One lives in the RTLS dashboard; the other gets buried in spreadsheets or a disconnected work order system. The problem surfaces fast during a Joint Commission survey, when inspectors don't just want to know where a ventilator is — they want a documented maintenance trail attached to it. The same applies to fixed life safety assets: medical gas shutoff valves, fire dampers, and smoke barriers all need location context and service history to satisfy survey requirements.
"The ability to link asset maintenance records directly to life safety drawings is critical for passing Joint Commission surveys without findings." — American Society for Health Care Engineering (ASHE)
Hospital inventory management software that can't bridge this gap forces facilities teams into a frantic pre-survey scramble — pulling records from multiple systems, cross-referencing paper logs, and hoping nothing has been missed. In practice, that gap is exactly where survey findings originate. Effective compliance management depends on records being instantly retrievable from the same interface used to locate an asset on a floorplan.
Proving 100% asset visibility — not just for movable equipment but for every life safety component mapped to an accurate drawing — is what transforms tracking from an operational convenience into a genuine compliance asset. The infrastructure to achieve that kind of unified visibility is what the next section addresses directly.
The Solution: A Centralized Healthcare Facility Hub
Fragmented FM tools create fragmented outcomes — and the antidote is a purpose-built hub that connects asset data, compliance workflows, and live floorplans in one place.
A unified healthcare facility hub eliminates the coordination gap that causes asset tracking to fail. Generic FM platforms weren't designed for hospital environments. They manage work orders, but they don't visualize PAR-level alerts on a live floorplan. They log maintenance records, but they don't connect those records to the architectural layout a surveyor reviews. The table below captures why that distinction matters:
- <strong>Generic FM Tools</strong>: Generic FM Tools | <strong>Healthcare-Specific Hub</strong>: Healthcare-Specific Hub
- <strong>Generic FM Tools</strong>: Static asset lists | <strong>Healthcare-Specific Hub</strong>: Assets visualized on live floorplans
- <strong>Generic FM Tools</strong>: Manual drawing updates | <strong>Healthcare-Specific Hub</strong>: Maintained Active Set — drawings kept current automatically
- <strong>Generic FM Tools</strong>: Siloed compliance logs | <strong>Healthcare-Specific Hub</strong>: Maintenance records linked to architectural context
- <strong>Generic FM Tools</strong>: Desktop-only access | <strong>Healthcare-Specific Hub</strong>: Mobile-first for bedside and on-floor inspections
- <strong>Generic FM Tools</strong>: No clinical system awareness | <strong>Healthcare-Specific Hub</strong>: Bridges facility data with EPIC RTLS workflows
Why Accurate Facility Data Is the Foundation of Asset Visibility
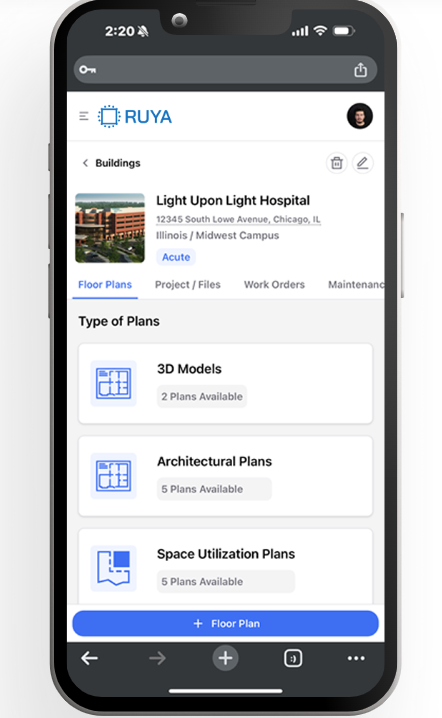
The Maintained Active Set is the operational core. Without a service that keeps CAD/BIM drawings continuously updated, every floorplan-based workflow drifts from reality. Ruya's mobile-accessible platform addresses this directly — combining CAD/BIM viewing with a Maintained Active Set service so teams are never working from outdated documentation.
Mobile-first inspections close the loop between field and record. ICRA and EOC workflows tied to asset data mean a technician walking the floor can confirm equipment status, flag an alert, and update a compliance record without returning to a workstation. PAR value thresholds visualized directly on the floorplan surface the right alerts at the right location — before a shortage becomes a care disruption.
When asset tracking, drawing accuracy, and compliance records share a single platform, the ROI becomes straightforward to demonstrate — which is exactly what the next section breaks down.
The Bottom Line: What You Need to Know
Active asset location management only delivers its full value when location data is anchored to accurate, current facility drawings — and that single insight reframes how hospital leaders should evaluate their entire tracking strategy.
The ROI case for asset tracking is well-documented. According to research on RTLS in healthcare, hospitals reclaim significant nursing hours previously lost to equipment searches, while reducing unnecessary capital purchases driven by "missing" assets that are simply mislocated. Those gains evaporate, however, when the underlying spatial data is stale.
RTLS must be anchored to a Maintained Active Set of drawings. Without it, location coordinates drift from physical reality over time — a problem that compounds with every renovation, equipment addition, or department reconfiguration. An infusion pump "located" in a wing that was converted eighteen months ago is effectively invisible to both clinical and compliance workflows.
Integration with systems like Epic matters for clinical efficiency, but it addresses a different problem. Workflow connectivity tells staff where assets are; facility-centric visualization tells compliance teams what has been done to those assets, and where. Compliance depends on linking maintenance records directly to architectural layouts — not just to device IDs floating in a database.
- Reclaimed nursing time is the most immediate ROI signal, but compliance risk reduction is the longer-term value driver.
- Spatial accuracy — not tag density — determines whether your RTLS investment survives a Joint Commission survey.
- Maintenance-to-layout linkage is the bridge between operational efficiency and defensible life safety compliance.
The question facing most system directors isn't whether to track assets, but whether their current strategy is built on a foundation stable enough to support it. That's the modernization conversation worth having next.
Modernizing Your Facility's Asset Strategy
Effective hospital asset tracking starts not with new hardware, but with an honest audit of the data foundation you already have. Before investing in RTLS sensors or barcode scanners, system directors should establish their current "ghost asset" rate — the percentage of recorded assets that can't be physically located or verified against an accurate floorplan. That number alone reveals whether a technology upgrade will deliver ROI or simply layer new costs onto an unreliable base.
The shift most facilities need is from hardware-first to data-first thinking. Research confirms that real-time location systems only perform reliably when asset records are tied to current, validated spatial data. Without that anchor, even sophisticated tracking platforms produce ghost assets and compliance gaps that erode clinical efficiency and regulatory standing.
Bridging BIM models with live compliance workflows is where many facilities stall — the technical gap between a design file and a working, inspection-ready document is wider than most teams anticipate. A specialized partner with purpose-built compliance features and BIM integration expertise can close that gap without burdening internal IT teams.
The practical next step for any system director is straightforward: centralize the floorplan as the single source of truth, then build asset data, compliance schedules, and life safety documentation outward from it. That sequence — drawing first, technology second — is what separates facilities that track assets from facilities that actually manage them.
Key Takeaways: Solving the Asset Tracking Gap
- Eliminate "Ghost Assets": Misplaced equipment costs a 200-bed hospital approximately $500,000 annually in lost nursing productivity. A robust tracking system can reduce redundant "safety stock" by over 20%.
- Data Drift is the Primary Failure Point: RTLS hardware is only as accurate as the floorplan it maps to. Static, outdated drawings render real-time location data misleading, creating "dead zones" during renovations.
- Integration vs. Visualization: While Epic manages patient workflows, it lacks native, facility-wide spatial visualization. Real-time location systems for hospitals require a dedicated facility-centric hub to bridge this data gap.
- Compliance Requires Context: Joint Commission surveys demand more than just location; they require a documented maintenance trail linked directly to architectural layouts (ASHE standards).
- The "Drawing-First" Strategy: To achieve true ROI, hospitals must prioritize a Maintained Active Set of floorplans as the authoritative foundation before scaling tracking technology.
Last updated: June 10, 2026

.png)
